




Definition
§ A
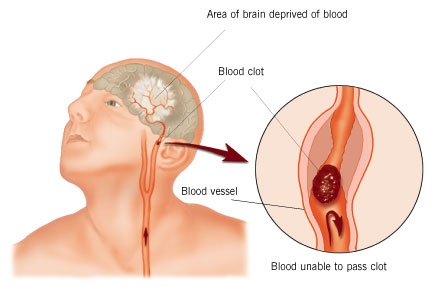
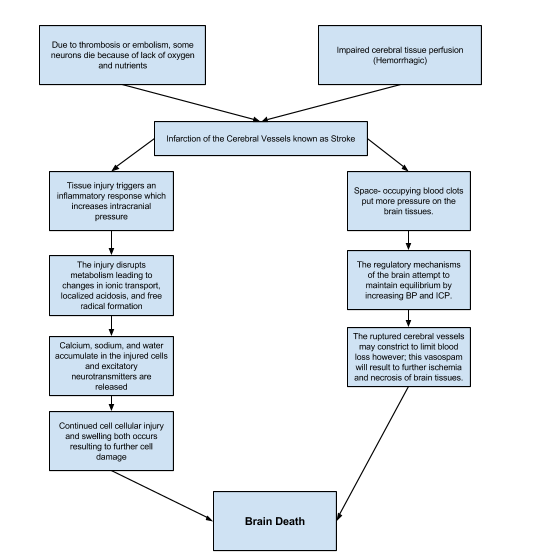
cerebrovascular accident (CVA), an ischemic stroke or “brain attack,” is a
sudden loss of brain function resulting from Cerebral Vascular Accident
(Ischemic Stroke) a disruption of the blood supply to a part of the brain.

Description
§ Stroke
is the primary cerebrovascular disorder in the United States.
§ Strokes are
usually hemorrhagic (15%) or ischemic/nonhemorrhagic (85%).
§ Ischemic
strokes are categorized according to their cause: large artery thrombotic
strokes (20%), small penetrating artery thrombotic strokes (25%),
cardiogenic embolic strokes (20%), cryptogenic strokes (30%), and other
(5%).
§ Cryptogenic
strokes have no known cause, and other strokes result from causes
such as illicit drug use, coagulopathies, migraine, and spontaneous
dissection of the carotid or vertebral arteries.
§ The result
is an interruption in the blood supply to the brain, causing temporary or permanent
loss of movement, thought, memory, speech, or sensation.
Risk Factors
Nonmodifable
§ Advanced
age (older than 55 years)
§ Gender
(Male)
§ Race
(African American)
Modifable
§ Hypertension
§ Atrial
fibrillation
§ Hyperlipidemia
§ Obesity
§ Smoking
§ Diabetes
§ Asymptomatic
carotid stenosis and valvular heart disease (eg, endocarditis, prosthetic
heart valves)
§ Periodontal
disease
Pathophysiology

Clinical Manifestations
General
signs and symptoms include numbness or weakness of face, arm, or leg
(especially on one side of body); confusion or change in mental status;
trouble speaking or understanding speech; visual disturbances; loss of
balance, dizziness, difficulty walking; or sudden severe headache.
Motor Loss
§ Hemiplegia,
hemiparesis
§ Flaccid
paralysis and loss of or decrease in the deep tendon reflexes (initial
clinical feature) followed by (after 48 hours) reappearance of deep
reflexes and abnormally increased muscle tone (spasticity)
Communication Loss
§ Dysarthria
(difficulty speaking)
§ Dysphasia
(impaired speech) or aphasia (loss of speech)
§ Apraxia
(inability to perform a previously learned action)
Perceptual Disturbances and Sensory
Loss
§ Visualperceptual
dysfunctions (homonymous hemianopia [loss of half of the visual field])
§ Disturbances
in visualspatial relations (perceiving the relation of two or more objects in
spatial areas), frequently seen in patients with right hemispheric damage
§ Sensory
losses: slight impairment of touch or more severe with loss of
proprioception; difficulty in interrupting visual, tactile, and auditory
stimuli
Impaired Cognitive and
Psychological Effects
§ Frontal
lobe damage: Learning capacity, memory, or other higher cortical
intellectual functions may be impaired. Such dysfunction may be reflected
in a limited attention span, difficulties in comprehension, forgetfulness, and
lack of motivation.
§ Depression,
other psychological problems: emotional lability, hostility, frustration,
resentment, and lack of cooperation.
Assessment
and Diagnostic Methods
§ History and
complete physical and neurologic examination
§ Noncontrast
CT scan
§ 12lead ECG
and carotid ultrasound
§ CT
angiography or MRI and angiography
§ Transcranial
Doppler flow studies
§ Transthoracic
or transesophageal echocardiography
§ Xenonenhanced
CT scan
§ Single
photon emission CT (SPECT) scan
Prevention
§ Help
patients alter risk factors for stroke; encourage patient to quit smoking,
maintain a healthy weight, follow a healthy diet (including modest alcohol
consumption), and exercise daily.
§ Prepare and
support patient through carotid endarterectomy.
§ Administer
anticoagulant agents as prescribed (eg, lowdose aspirin therapy).
Medical Management
§ Recombinant
tissue plasminogen activator (tPA), unless contraindicated; monitor for
bleeding
§ Anticoagulation
therapy
§ Management
of increased intracranial pressure (ICP): osmotic diuretics, maintain
PaCO2 at 30 to 35 mm Hg, position to avoid hypoxia (elevate the head of bed to
promote venous drainage and to lower increased ICP)
§ Possible
hemicraniectomy for increased ICP from brain edema in a very large stroke
§ Intubation
with an endotracheal tube to establish a patent airway, if necessary
§ Continuous
hemodynamic monitoring (the goals for blood pressure remain controversial
for a patient who has not received thrombolytic therapy; antihypertensive
treatment may be withheld unless the systolic blood pressure
exceeds mm Hg or the diastolic blood pressure exceeds 120 mm Hg)
§ Neurologic
assessment to determine if the stroke is evolving and if other acute
complications are developing
Management of Complications
§ Decreased
cerebral blood flow: Pulmonary care, maintenance of a patent airway, and
administration of supplemental oxygen as needed.
§ Monitor for
UTIs, cardiac dysrhythmias, and complications of immobility.
Nursing Assessment
During Acute Phase (1 to 3 days)
Weigh
patient (used to determine medication dosages), and maintain a neurologic
flow sheet to reflect the following nursing assessment parameters:
§ Change in
level of consciousness or responsiveness, ability to speak, and
orientation
§ Presence or
absence of voluntary or involuntary movements of the extremities: muscle
tone, body posture, and head position
§ Stiffness
or flaccidity of the neck
§ Eye
opening, comparative size of pupils and pupillary reactions to light, and
ocular position
§ Color of
face and extremities; temperature and moisture of skin
§ Quality and
rates of pulse and respiration; ABGs, body temperature, and arterial
pressure
§ Volume of
fluids ingested or administered and volume of urine excreted per 24 hours
§ Signs of
bleeding
§ Blood
pressure maintained within normal limits
Postacute
Phase
Assess
the following functions:
§ Mental
status (memory, attention span, perception, orientation, affect,
speech/language).
§ Sensation
and perception (usually the patient has decreased awareness of pain and
temperature).
§ Motor
control (upper and lower extremity movement); swallowing ability,
nutritional and hydration status, skin integrity, activity tolerance, and
bowel and bladder function.
§ Continue
focusing nursing assessment on impairment of function in patient’s daily
activities.
Diagnosis
Nursing Diagnoses
§ Impaired
physical mobility related to hemiparesis, loss of balance and
coordination, spasticity, and brain injury
§ Acute pain
related to hemiplegia and disuse
§ Deficient
selfcare (bathing, hygiene, toileting, dressing, grooming, and feeding)
related to stroke sequelae
§ Disturbed
sensory perception (kinesthetic, tactile, or visual) related to altered
sensory reception, transmission, and/or integration
§ Impaired
swallowing
§ Impaired
urinary elimination related to flaccid bladder, detrusor instability,
confusion, or difficulty in communicating
§ Disturbed
thought processes related to brain damage
§ Impaired
verbal communication related to brain damage
§ Risk for
impaired skin integrity related to hemiparesis or hemiplegia, decreased
mobility
§ Interrupted
family processes related to catastrophic illness and caregiving burdens
§ Sexual
dysfunction related to neurologic deficits or fear of failure
Collaborative Problems/Potential
Complications
§ Decreased
cerebral blood flow due to increased ICP; inadequate oxygen delivery to the
brain; pneumonia.
Planning and Goals
The
major goals for the patient (and family) may include improved mobility,
avoidance of shoulder pain, achievement of selfcare, relief of sensory and
perceptual deprivation, prevention of aspiration, continence of bowel and
bladder, improved thought processes, achieving a form of communication,
maintaining skin integrity, restored family functioning, improved sexual
function, and absence of complications. Goals are affected by knowledge of
what the patient was like before the stroke.
Nursing Interventions
Improving Mobility and Preventing Deformities
§ Position to
prevent contractures; use measures to relieve pressure, assist in
maintaining good body alignment, and prevent compressive neuropathies.
§ Apply a
splint at night to prevent flexion of affected extremity.
§ Prevent
adduction of the affected shoulder with a pillow placed in the axilla.
§ Elevate
affected arm to prevent edema and fibrosis.
§ Position
fingers so that they are barely flexed; place hand in slight supination. If
upper extremity spasticity is noted, do not use a hand roll; dorsal wrist
splint may be used.
§ Change
position every 2 hours; place patient in a prone position for 15 to 30
minutes several times a day.
Establishing an Exercise Program
§ Provide
full range of motion four or five times a day to maintain joint mobility,
regain motor control, prevent contractures in the paralyzed extremity,
prevent further deterioration of the neuromuscular system, and
enhance circulation. If tightness occurs in any area, perform
rangeofmotion exercises more frequently.
§ Exercise is
helpful in preventing venous stasis, which may predispose the patient to
thrombosis and pulmonary embolus.
§ Observe for
signs of pulmonary embolus or excessive cardiac workload during exercise period
(eg, shortness of breath, chest pain, cyanosis, and increasing pulse
rate).
§ Supervise
and support patient during exercises; plan frequent short periods of
exercise, not longer periods; encourage patient to exercise unaffected
side at intervals throughout the day.
Preparing for Ambulation
§ Start an
active rehabilitation program when consciousness returns (and all evidence
of bleeding is gone, when indicated).
§ Teach
patient to maintain balance in a sitting position, then to balance while
standing (use a tilt table if needed).
§ Begin
walking as soon as standing balance is achieved (use parallel bars and
have wheelchair available in anticipation of possible dizziness).
§ Keep
training periods for ambulation short and frequent.
NURSING
ALERT: Initiate a full rehabilitation program even for
elderly patients.
Preventing Shoulder Pain
§ Never lift
patient by the flaccid shoulder or pull on the affected arm or shoulder.
§ Use proper
patient movement and positioning (eg, flaccid arm on a table or pillows
when patient is seated, use of sling when ambulating).
§ Rangeofmotion
exercises are beneficial, but avoid overstrenuous arm movements.
§ Elevate arm
and hand to prevent dependent edema of the hand; administer analgesic
agents as indicated.
Enhancing Self Care
§ Encourage
personal hygiene activities as soon as the patient can sit up; select
suitable selfcare activities that can be carried out with one hand.
§ Help
patient to set realistic goals; add a new task daily.
§ As a first
step, encourage patient to carry out all selfcare activities on the
unaffected side.
§ Make sure
patient does not neglect affected side; provide assistive devices as
indicated.
§ Improve
morale by making sure patient is fully dressed during ambulatory
activities.
§ Assist with
dressing activities (eg, clothing with Velcro closures; put garment on the
affected side first); keep environment uncluttered and organized.
§ Provide
emotional support and encouragement to prevent fatigue and discouragement.
Managing Sensory Perceptual
Difficulties
§ Approach
patient with a decreased field of vision on the side where visual
perception is intact; place all visual stimuli on this side.
§ Teach
patient to turn and look in the direction of the defective visual field to
compensate for the loss; make eye contact with patient, and draw attention
to affected side.
§ Increase
natural or artificial lighting in the room; provide eyeglasses to improve
vision.
§ Remind
patient with hemianopsia of the other side of the body; place extremities
so that patient can see them.
Assisting with Nutrition
§ Observe
patient for paroxysms of coughing, food dribbling out or pooling in one
side of the mouth, food retained for long periods in the mouth, or nasal
regurgitation when swallowing liquids.
§ Consult
with speech therapist to evaluate gag reflexes; assist in teaching
alternate swallowing techniques, advise patient to take smaller boluses of
food, and inform patient of foods that are easier to swallow; provide
thicker liquids or pureed diet as indicated.
§ Have
patient sit upright, preferably on chair, when eating and drinking;
advance diet as tolerated.
§ Prepare for
GI feedings through a tube if indicated; elevate the head of bed during
feedings, check tube position before feeding, administer feeding slowly, and
ensure that cuff of tracheostomy tube is inflated (if
applicable); monitor and report excessive retained or residual feeding.
Attaining Bowel and Bladder Control
§ Perform
intermittent sterile catheterization during period of loss of sphincter
control.
§ Analyze
voiding pattern and offer urinal or bedpan on patient’s voiding schedule.
§ Assist the
male patient to an upright posture for voiding.
§ Provide
highfiber diet and adequate fluid intake (2 to 3 L/day), unless
contraindicated.
§ Establish a
regular time (after breakfast) for toileting.
Improving Thought Processes
§ Reinforce
structured training program using cognitiveperceptual retraining, visual
imagery, reality orientation, and cueing procedures to compensate for
losses.
§ Support
patient: Observe performance and progress, give positive feedback, convey
an attitude of confidence and hopefulness; provide other interventions as
used for improving cognitive function after a head injury.
Improving Communication
§ Reinforce
the individually tailored program.
§ Jointly
establish goals, with patient taking an active part.
§ Make the
atmosphere conducive to communication, remaining sensitive to patient’s
reactions and needs and responding to them in an appropriate manner;
treat patient as an adult.
§ Provide
strong emotional support and understanding to allay anxiety; avoid
completing patient’s sentences.
§ Be
consistent in schedule, routines, and repetitions. A written schedule,
checklists, and audiotapes may help with memory and concentration; a communication
board may be used.
§ Maintain
patient’s attention when talking with patient, speak slowly, and give one
instruction at a time; allow patient time to process.
§ Talk to
aphasic patients when providing care activities to provide social contact.
Maintaining Skin Integrity
§ Frequently
assess skin for signs of breakdown, with emphasis on bony areas and dependent
body parts.
§ Employ
pressurerelieving devices; continue regular turning and positioning (every 2
hours minimally); minimize shear and friction when positioning.
§ Keep skin
clean and dry, gently massage healthy dry skin, and maintain adequate
nutrition.
Improving Family Coping
§ Provide
counseling and support to family.
§ Involve
others in patient’s care; teach stress management techniques and
maintenance of personal health for family coping.
§ Give family
information about the expected outcome of the stroke, and counsel them to
avoid doing things for patient that he or she can do.
§ Develop
attainable goals for patient at home by involving the total health care team,
patient, and family.
§ Encourage
everyone to approach patient with a supportive and optimistic attitude,
focusing on abilities that remain; explain to family that emotional
lability usually improveswith time.
Helping the Patient Cope with
Sexual Dysfunction
§ Perform
indepth assessment to determine sexual history before and after the
stroke.
§ Interventions
for patient and partner focus on providing relevant information,
education, reassurance, adjustment
§ of
medications, counseling regarding coping skills, suggestions for alternative
sexual positions, and a means of sexual expression and satisfaction.
Teaching Points
§ Teach
patients about the “act FAST” Campaign
§ Teach
patient to resume as much selfcare as possible; provide assistive devices as
indicated.
§ Have occupational
therapist make a home assessment and recommendations to help patient
become more independent.
§ Coordinate
care provided by numerous health care professionals; help family plan aspects
of care.
§ Advise
family that patient may tire easily, become irritable and upset by small
events, and show less interest in daily events.
§ Make
referral for home speech therapy. Encourage family involvement. Provide
family with practical instructions to help patient between speech therapy
sessions.
§ Discuss
patient’s depression with physician for possible antidepressant therapy.
§ Encourage
patient to attend communitybased stroke clubs to give a feeling of
belonging and fellowship with others.
§ Encourage
patient to continue with hobbies, recreational and leisure interests, and
contact with friends to prevent social isolation.
§ Encourage
family to support patient and give positive reinforcement.
§ Remind
spouse and family to attend to personal health and wellbeing.
Evaluation
Expected Patient Outcomes
§ Achieves
improved mobility.
§ Has no
complaints of pain.
§ Achieves
selfcare; performs hygiene care; uses adaptive equipment.
§ Demonstrates
techniques to compensate for altered sensory reception, such as turning
the head to see people or objects.
§ Demonstrates
safe swallowing.
§ Achieves
normal bowel and bladder elimination.
§ Participates
in cognitive improvement program.
§ Demonstrates
improved communication.
§ Maintains
intact skin without breakdown.
§ Family
members demonstrate a positive attitude and coping mechanisms.
§ Develops
alternative approaches to sexual expression.
Nursing
Care Plan
Nursing Diagnosis
§ Ineffective
Cerebral Tissue Perfusion
May be related to
§ Interruption
of blood flow: occlusive disorder, hemorrhage; cerebral vasospasm, cerebral
edema
Possibly evidenced by
§ Altered
level of consciousness; memory loss
§ Changes
in motor/sensory responses; restlessness
§ Sensory,
language, intellectual, and emotional deficits
§ Changes
in vital signs
Desired Outcomes
§ Maintain
usual/improved level of consciousness, cognition, and motor/sensory function.
§ Demonstrate
stable vital signs and absence of signs of increased ICP.
§ Display
no further deterioration/recurrence of deficits
Nursing Interventions
§ Assess
factors related to individual situation for decreased cerebral perfusion and
potential for increased ICP.
§ Rationale: Assessment
will determine and influence the choice of interventions. Deterioration in
neurological signs or failure to improve after initial insult may reflect
decreased intracranial adaptive capacity requiring patient to be transferred to
critical area for monitoring of ICP, other therapies. If the stroke is
evolving, patient can deteriorate quickly and require repeated assessment and
progressive treatment. If the stroke is “completed,” the neurological deficit
is nonprogressive, and treatment is geared toward rehabilitation and preventing
recurrence.
§ Closely
assess and monitor neurological status frequently and compare with baseline.
§ Rationale: Assesses
trends in level of consciousness (LOC) and potential for increased ICP and is
useful in determining location, extent, and progression of damage. May also
reveal presence of TIA, which may warn of impending thrombotic CVA.
Monitor vital
signs:
§ changes
in blood pressure, compare BP readings in both arms.
§ Rationale: Fluctuations
in pressure may occur because of cerebral injury in vasomotor area of the brain. Hypertension or postural hypotension may have been a
precipitating factor. Hypotension may
occur because of shock (circulatory collapse). Increased ICPmay occur because of tissue edema or clot
formation. Subclavian artery
blockage may be revealed by difference in pressure readings between
arms.
§ Heart
rate and rhythm, assess for murmurs.
§ Rationale: Changes
in rate, especially bradycardia, can occur because of the brain damage.
Dysrhythmias and murmurs may reflect cardiac disease, which may have
precipitated CVA (stroke after MI or from valve dysfunction).
§ Respirations,
noting patterns and rhythm (periods of apnea after hyperventilation),
Cheyne-Stokes respiration.
§ Rationale: Irregularities
can suggest location of cerebral insult or increasing ICP and need
for further intervention, including possible respiratory support.
§ Evaluate
pupils, noting size, shape, equality, light reactivity.
§ Rationale: Pupil
reactions are regulated by the oculomotor (III) cranial nerve and are useful in
determining whether the brain stem is intact. Pupil size and equality is
determined by balance between parasympathetic and sympathetic innervation.
Response to light reflects combined function of the optic (II) and oculomotor
(III) cranial nerves.
§ Document
changes in vision: reports of blurred vision, alterations in visual field,
depth perception.
§ Rationale: Specific
visual alterations reflect area of brain involved, indicate safety concerns,
and influence choice of interventions.
§ Assess
higher functions, including speech, if patient is alert.
§ Rationale: Changes
in cognition and speech content are an indicator of location and degree of
cerebral involvement and may indicate deterioration or increased ICP.
§ Position
with head slightly elevated and in neutral position.
§ Rationale: Reduces
arterial pressure by promoting venous drainage and may improve cerebral
perfusion.
§ Maintain
bedrest, provide quiet and relaxing environment, restrict visitors and
activities. Cluster nursing interventions and provide rest periods between care
activities. Limit duration of procedures.
§ Rationale: Continuous
stimulation or activity can increase intracranial pressure (ICP). Absolute
rest and quiet may be needed to prevent rebleeding in the case of hemorrhage.
§ Prevent
straining at stool, holding breath.
§ Rationale: Valsalva
maneuver increases ICP and potentiates risk of rebleeding.
§ Assess
for nuchal rigidity, twitching, increased restlessness, irritability, onset of
seizure activity.
§ Rationale: Indicative
of meningeal irritation, especially in hemorrhage disorders. Seizures may
reflect increased ICP or cerebral injury, requiring further evaluation and
intervention.
§ Administer
supplemental oxygen as indicated.
§ Rationale: Reduces
hypoxemia. Hypoxemia can cause cerebral vasodilation and increase pressure or
edema formation.
Administer medications as
indicated:
§ Alteplase
(Activase), t-PA;
§ Rationale: Thrombolytic
agents are useful in dissolving clot when started within 3 hr of initial
symptoms. Thirty percent are likely to recover with little or no disability.
Treatment is based on trying to limit the size of the infarct, and use requires
close monitoring for signs of intracranial hemorrhage. Note: These agents
are contraindicated in cranial hemorrhage as diagnosed by CT scan.
§ Anticoagulants: warfarin sodium
(Coumadin), low-molecular-weight heparin (Lovenox);
§ Rationale: May
be used to improve cerebral blood flow and prevent further clotting when
embolism and/or thrombosis is the problem.
§ Antiplatelet agents: aspirin (ASA),
dipyridamole (Persantine), ticlopidine (Ticlid);
§ Rationale: Contraindicated
in hypertensive patients because of increased risk of hemorrhage.
§ Antifibrinolytics: aminocaproic acid
(Amicar);
§ Rationale: Used
with caution in hemorrhagic disorder to prevent lysis of formed clots and
subsequent rebleeding.
§ Antihypertensives
§ Rationale: Chronic
hypertension requires cautious treatment because aggressive management
increases the risk of extension of tissue damage.
§ Peripheral vasodilators: cyclandelate
(Cyclospasmol), papaverine (Pavabid), isoxsuprine (Vasodilan).
§ Rationale: Transient
hypertension often occurs during acute stroke and resolves often without
therapeutic intervention.Used to improve collateral circulation or decrease
vasospasm.
§ Steroids: dexamethasone (Decadron).
§ Rationale: Use
is controversial in control of cerebral edema.
§ Neuroprotective agents: calcium channel blockers,
excitatory amino acid inhibitors, gangliosides.
§ Rationale: These
agents are being researched as a means to protect the brain by interrupting the
destructive cascade of biochemical events (influx of calcium into cells,
release of excitatory neurotransmitters, buildup of lactic acid) to limit
ischemic injury.
§ Phenytoin
(Dilantin), phenobarbital.
§ Rationale: May
be used to control seizures and/or for sedative action. Note:
Phenobarbital enhances action of antiepileptics.
§ Stool
softeners.
§ Rationale: Prevents
straining during bowel movement and corresponding increase of ICP.
§ Prepare
for surgery, as appropriate: endarterectomy, microvascular bypass, cerebral
angioplasty.
§ Rationale: May
be necessary to resolve situation, reduce neurological symptoms of recurrent
stroke.
§ Monitor
laboratory studies as indicated: prothrombin time (PT) and/or activated
partial thromboplastin time (aPTT) time, Dilantin level.
§ Rationale: Provides
information about drug effectiveness and/or therapeutic level.
Nursing Diagnosis
§ Impaired
Physical Mobility
May be related to
§ Neuromuscular
involvement: weakness, paresthesia; flaccid/hypotonic paralysis (initially);
spastic paralysis
§ Perceptual/cognitive
impairment
Possibly evidenced by
§ Inability
to purposefully move within the physical environment; impaired coordination;
limited range of motion; decreased muscle strength/control
Desired Outcomes
§ Maintain/increase
strength and function of affected or compensatory body part.
§ Maintain
optimal position of function as evidenced by absence of contractures, foot
drop.
§ Demonstrate
techniques/behaviors that enable resumption of activities.
§ Maintain
skin integrity.
Nursing Interventions
§ Assess
extent of impairment initially and on a regular basis. Classify according to
0–4 scale.
§ Rationale: Identifies
strengths and deficiencies that may provide information regarding
recovery. Assists in choice of interventions, because different techniques are
used for flaccid and spastic paralysis.
§ Change
positions at least every 2 hr (supine, side lying) and possibly more often if
placed on affected side.
§ Rationale: Reduces
risk of tissue injury. Affected side has poorer circulation and reduced
sensation and is more predisposed to skin breakdown.
§ Position
in prone position once or twice a day if patient can tolerate.
§ Rationale: Helps
maintain functional hip extension; however, may increase anxiety, especially
about ability to breathe.
§ Prop
extremities in functional position; use footboard during the period of flaccid
paralysis. Maintain neutral position of head.
§ Rationale: Prevents
contractures and footdrop and facilitates use when function returns. Flaccid
paralysis may interfere with ability to support head, whereas spastic paralysis
may lead to deviation of head to one side.
§ Use arm
sling when patient is in upright position, as indicated.
§ Rationale: During
flaccid paralysis, use of sling may reduce risk of shoulder subluxation and
shoulder-hand syndrome.
§ Evaluate
need for positional aids and/or splints during spastic paralysis:
§ Rationale: Flexion
contractures occur because flexor muscles are stronger than extensors.
§ Place
pillow under axilla to abduct arm
§ Rationale: Prevents
adduction of shoulder and flexion of elbow.
§ Elevate
arm and hand
§ Rationale: Promotes
venous return and helps prevent edema formation.
§ Place
hard hand-rolls in the palm with fingers and thumb opposed.
§ Rationale: Hard
cones decrease the stimulation of finger flexion, maintaining finger and thumb
in a functional position.
§ Place
knee and hop in extended position;
§ Rationale: Maintains
functional position.
§ Maintain
leg in neutral position with a trochanter roll;
§ Rationale: Prevents
external hip rotation.
§ Discontinue
use of footboard, when appropriate.
§ Rationale: Continued
use (after change from flaccid to spastic paralysis) can cause excessive
pressure on the ball of the foot, enhance spasticity, and actually increase
plantar flexion.
§ Observe
affected side for color, edema, or other signs of compromised circulation.
§ Rationale: Edematous
tissue is more easily traumatized and heals more slowly.
§ Inspect
skin regularly, particularly over bony prominences. Gently massage any reddened
areas and provide aids such as sheepskin pads as necessary.
§ Rationale: Pressure
points over bony prominences are most at risk for decreased perfusion.
Circulatory stimulation and padding help prevent skin breakdown and decubitus
development.
§ Begin
active or passive ROM to all extremities (including splinted) on admission.
Encourage exercises such as quadriceps/gluteal exercise, squeezing rubber ball,
extension of fingers and legs/feet.
§ Rationale: Minimizes
muscle atrophy, promotes circulation, helps prevent contractures. Reduces risk
of hypercalciuria and osteoporosis if underlying problem is hemorrhage. Note:
Excessive stimulation can predispose to rebleeding.
§ Assist
patient with exercise and perform ROM exercises for both the affected and
unaffected sides. Teach and encourage patient to use his unaffected side to
exercise his affected side.
§ Assist
patient to develop sitting balance by raising head of bed, assist to sit on
edge of bed, having patient to use the strong arm to support body weight and
move using the strong leg. Assist to develop standing balance by putting flat
walking shoes, support patient’s lower back with hands while positioning own
knees outside patient’s knees, assist in using parallel bars.
§ Rationale:Aids
in retraining neuronal pathways, enhancing proprioception and motor response.
§ Get
patient up in chair as soon as vital signs are stable, except following
cerebral hemorrhage.
§ Rationale:Helps
stabilize BP (by restoring vasomotor tone), promotes maintenance of extremities
in a functional position and emptying of bladder, reducing risk of urinary
stones and infections from stasis. Note: If stroke is not completed,
activity increases risk of additional bleed.
§ Pad
chair seat with foam or water-filled cushion, and assist patient to shift
weight at frequent intervals.
§ Rationale: To
prevent pressure on the coccyx and skin breakdown.
§ Set
goals with patient and SO for participation in activities and position changes.
§ Rationale: Promotes
sense of expectation of improvement, and provides some sense of control and
independence.
§ Encourage
patient to assist with movement and exercises using unaffected extremity to
support and move weaker side.
§ Rationale: May
respond as if affected side is no longer part of body and needs encouragement
and active training to “reincorporate” it as a part of own body.
§ Provide
egg-crate mattress, water bed, flotation device, or specialized beds, as
indicated.
§ Rationale: Promotes
even weight distribution, decreasing pressure on bony points and helping to
prevent skin breakdown and decubitus formation. Specialized beds help with
positioning, enhance circulation, and reduce venous stasis to decrease risk of
tissue injury and complications such as orthostatic pneumonia.
§ Position
the patient and align his extremities correctly. Use high-top sneakers to
prevent footdrop and contracture and convoluted foam, flotation, or pulsating
mattresses or sheepskin.
§ Rationale: These
are measures to prevent pressure ulcers.
Nursing Diagnosis
§ Communication,
impaired verbal [and/or written]
May be related to
§ Impaired
cerebral circulation; neuromuscular impairment, loss of facial/oral muscle
tone/control; generalized weakness/fatigue
Possibly evidenced by
§ Impaired
articulation; does not/cannot speak (dysarthria)
§ Inability
to modulate speech, find and name words, identify objects; inability to
comprehend written/spoken language
§ Inability
to produce written communication
Desired Outcomes
§ Indicate
an understanding of the communication problems.
§ Establish
method of communication in which needs can be expressed.
§ Use resources
appropriately.
Nursing Interventions
§ Assess
extent of dysfunction: patient cannot understand words or has trouble
speaking or making self understood. Differentiate aphasia from dysarthria.
§ Rationale: Helps
determine area and degree of brain involvement and difficulty patient has with
any or all steps of the communication process. Patient may have receptive aphasia or damage to the
Wernicke’s speech area which is characterized by difficulty of understanding
spoken words. He may also have expressive
aphasia or damage to the Broca’s speech areas, which is difficulty in
speaking words correctly, or may experience both. Choice of interventions
depends on type of impairment. Aphasia is
a defect in using and interpreting symbols of language and may involve sensory
and/or motor components (inability to comprehend written and/or spoken words or
to write, make signs, speak). A dysarthric person
can understand, read, and write language but has difficulty forming and
pronouncing words because of weakness and paralysis of oral musculature.
Patient may lose ability to monitor verbal output and be unaware that
communication is not sensible.
§ Listen
for errors in conversation and provide feedback.
§ Rationale: Feedback
helps patient realize why caregivers are not understanding or responding
appropriately and provides opportunity to clarify meaning.
§ Ask
patient to follow simple commands (“Close and open your eyes,” “Raise your
hand”); repeat simple words or sentences;
§ Rationale: Tests
for receptive aphasia.
§ Point
to objects and ask patient to name them.
§ Rationale: Tests
for expressive aphasia. Patient may recognize item but not be able to name it.
§ Have
patient produce simple sounds (“Dog,” “meow,” “Shh”).
§ Rationale: Identifies
dysarthria, because motor components of speech (tongue, lip movement, breath
control) can affect articulation and may or may not be accompanied by
expressive aphasia.
§ Ask
patient to write his name and a short sentence. If unable to write, have
patient read a short sentence.
§ Rationale: Tests
for writing disability (agraphia) and deficits in reading comprehension
(alexia), which are also part of receptive and expressive aphasia.
§ Write a
notice at the nurses’ station and patient’s room about speech impairment.
Provide a special call bell that can be activated by minimal pressure if
necessary.
§ Rationale: Allays
anxiety related to inability to communicate and fear that needs will not be met
promptly.
§ Provide
alternative methods of communication: writing, pictures.
§ Rationale: Provides
communication needs of patient based on individual situation and underlying
deficit.
§ Anticipate
and provide for patient’s needs.
§ Rationale: Helpful
in decreasing frustration when dependent on others and unable to communication
desires.
§ Talk
directly to patient, speaking slowly and distinctly. Phrase questions to be
answered simply by yes or no. Progress in complexity as patient responds.
§ Rationale: Reduces
confusion and allays anxiety at having to process and respond to large amount
of information at one time. As retraining progresses, advancing complexity of
communication stimulates memory and further enhances word and idea association.
§ Speak
in normal tones and avoid talking too fast. Give patient ample time to respond.
Avoid pressing for a response.
§ Rationale: Patient
is not necessarily hearing impaired, and raising voice may irritate or anger
patient. Forcing responses can result in frustration and may cause patient to
resort to “automatic” speech (garbled speech, obscenities).
§ Encourage
SO/visitors to persist in efforts to communicate with patient: reading mail,
discussing family happenings even if patient is unable to respond
appropriately.
§ Rationale: It
is important for family members to continue talking to patient to reduce
patient’s isolation, promote establishment of effective communication, and
maintain sense of connectedness with family.
§ Discuss
familiar topics, e.g., weather, family, hobbies, jobs.
§ Rationale: Promotes
meaningful conversation and provides opportunity to practice skills.
§ Respect
patient’s preinjury capabilities; avoid “speaking down” to patient or making
patronizing remarks.
§ Rationale: Enables
patient to feel esteemed, because intellectual abilities often remain intact.
§ Consult
and refer patient to speech therapist.
§ Rationale: Assesses
individual verbal capabilities and sensory, motor, and cognitive functioning to
identify deficits/therapy needs.
Nursing Diagnosis
§ Disturbed
Sensory Perception
May be related to
§ Altered
sensory reception, transmission, integration (neurological trauma or deficit)
§ Psychological
stress (narrowed perceptual fields caused by anxiety)
Possibly evidenced by
§ Disorientation
to time, place, person
§ Change
in behavior pattern/usual response to stimuli; exaggerated emotional responses
§ Poor
concentration, altered thought processes/bizarre thinking
§ Reported/measured
change in sensory acuity: hypoparesthesia; altered sense of taste/smell
§ Inability
to tell position of body parts (proprioception)
§ Inability
to recognize/attach meaning to objects (visual agnosia)
§ Altered
communication patterns
§ Motor
incoordination
Desired Outcomes
§ Regain/maintain
usual level of consciousness and perceptual functioning.
§ Acknowledge
changes in ability and presence of residual involvement.
§ Demonstrate
behaviors to compensate for/overcome deficits.
Nursing Interventions
§ Review
pathology of individual condition.
§ Rationale: Awareness
on the type and areas of involvement aid in assessing specific deficit and
planning of care.
§ Observe
behavioral responses: crying, inappropriate affect, agitation, hostility,
agitation, hallucination.
§ Rationale: Individual
responses are variable, but commonalities such as emotional lability, lowered
frustration threshold, apathy, and impulsiveness may complicate care.
§ Establish
and maintain communication with the patient. Set up a simple method of communicating
basic needs. Remember to phrase your questions so he’ll be able to answer using
this system. Repeat yourself quietly and calmly and use gestures when necessary
to help in understanding.
§ Rationale: Note:
even an unresponsive patient may be able to hear, so don’t say anything in his
presence you wouldn’t want him to hear and remember.
§ Eliminate
extraneous noise and stimuli as necessary.
§ Rationale: Reduces
anxiety and exaggerated emotional responses and confusion associated with
sensory overload.
§ Speak
in calm, comforting, quiet voice, using short sentences. Maintain eye contact.
§ Rationale: Patient
may have limited attention span or problems with comprehension. These measures
can help patient attend to communication.
§ Ascertain
patient’s perceptions. Reorient patient frequently to environment, staff,
procedures.
§ Rationale: Assists
patient to identify inconsistencies in reception and integration of stimuli and
may reduce perceptual distortion of reality.
§ Evaluate
for visual deficits. Note loss of visual field, changes in depth perception
(horizontal and/or vertical planes), presence of diplopia (double vision).
§ Rationale: Presence
of visual disorders can negatively affect patient’s ability to perceive
environment and relearn motor skills and increases risk of accident and injury.
§ Approach
patient from visually intact side. Leave light on; position objects to take
advantage of intact visual fields. Patch affected eye if indicated.
§ Rationale: Helps
the patient to recognize the presence of persons or objects and may help with
depth perception problems. This also prevents patient from being startled.
Patching the eye may decrease sensory confusion of double vision.
§ Assess
sensory awareness: dull from sharp, hot from cold, position of body parts,
joint sense.
§ Rationale: Diminished
sensory awareness and impairment of kinesthetic sense negatively affects
balance and positioning and appropriateness of movement, which
interferes with ambulation, increasing risk of trauma.
§ Stimulate
sense of touch. Give patient objects to touch, and hold. Have patient
practice touching walls boundaries.
§ Rationale: Aids
in retraining sensory pathways to integrate reception and interpretation of
stimuli. Helps patient orient self spatially and strengthens use of affected
side.
§ Protect
from temperature extremes; assess environment for hazards. Recommend testing
warm water with unaffected hand.
§ Rationale: Promotes
patient safety, reducing risk of injury.
§ Note
inattention to body parts, segments of environment, lack of recognition of
familiar objects/persons.
§ Rationale: Agnosia,
the loss of comprehension of auditory, visual, or other sensations, may lead
result to unilateral neglect, inability to recognize environmental cues,
considerable self-care deficits, and disorientation or bizarre behavior.
§ Encourage
patient to watch feet when appropriate and consciously position body parts.
Make patient aware of all neglected body parts: sensory stimulation to affected
side, exercises that bring affected side across midline, reminding person to
dress/care for affected (“blind”) side.
§ Rationale: Use
of visual and tactile stimuli assists in reintegration of affected side and
allows patient to experience forgotten sensations of normal movement patterns.
Nursing Diagnosis
§ Ineffective
Coping
May be related to
§ Situational
crises, vulnerability, cognitive perceptual changes
Possibly evidenced by
§ Inappropriate
use of defense mechanisms
§ Inability
to cope/difficulty asking for help
§ Change
in usual communication patterns
§ Inability
to meet basic needs/role expectations
§ Difficulty
problem solving
Desired Outcomes
§ Verbalize
acceptance of self in situation.
§ Talk/communicate
with SO about situation and changes that have occurred.
§ Verbalize
awareness of own coping abilities.
§ Meet
psychological needs as evidenced by appropriate expression of feelings,
identification of options, and use of resources.
Nursing Interventions
§ Assess
extent of altered perception and related degree of disability. Determine
Functional Independence Measure score.
§ Rationale: Determination
of individual factors aids in developing plan of care/choice of interventions
and discharge expectations.
§ Identify
meaning of the dysfunction and change to patient. Note ability to understand
events, provide realistic appraisal of the situation.
§ Rationale: Independence
is highly valued in American culture but is not as significant in some
cultures. Some patients accept and manage altered function effectively with
little adjustment, whereas others may have considerable difficulty recognizing
and adjust to deficits. In order to provide meaningful support and
appropriate problem-solving, healthcare providers need to understand the
meaning of the stroke/limitations to patient.
§ Determine
outside stressors: family, work, future healthcare needs.
§ Rationale: Helps
identify specific needs, provides opportunity to offer information and begin
problem-solving. Consideration of social factors, in addition to functional
status, is important in determining appropriate discharge destination.
§ Provide
psychological support and set realistic short-term goals. Involve the patient’s
SO in plan of care when possible and explain his deficits and strengths.
§ Rationale: To
increase the patient’s sense of confidence and can help in compliance to
therapeutic regimen.
§ Encourage
patient to express feelings, including hostility or anger, denial, depression,
sense of disconnectedness.
§ Rationale: Demonstrates
acceptance of patient in recognizing and beginning to deal with these
feelings.
§ Note
whether patient refers to affected side as “it” or denies affected side and
says it is “dead.”
§ Rationale: Suggests
rejection of body part and negative feelings about body image and abilities,
indicating need for intervention and emotional support.
§ Acknowledge
statement of feelings about betrayal of body; remain matter-of-fact about
reality that patient can still use unaffected side and learn to control
affected side. Use words (weak, affected, right-left) that incorporate that
side as part of the whole body.
§ Rationale: Helps
patient see that the nurse accepts both sides as part of the whole individual.
Allows patient to feel hopeful and begin to accept current situation.
§ Identify
previous methods of dealing with life problems. Determine presence of
support systems.
§ Rationale: Provides
opportunity to use behaviors previously effective, build on past successes, and
mobilize resources.
§ Emphasize
small gains either in recovery of function or independence.
§ Rationale: Consolidates
gains, helps reduce feelings of anger and helplessness, and conveys sense of
progress.
§ Support
behaviors and efforts such as increased interest/participation in
rehabilitation activities.
§ Rationale: Suggest
possible adaptation to changes and understanding about own role in future
lifestyle.
§ Monitor
for sleep disturbance, increased difficulty concentrating, statements of
inability to cope, lethargy, withdrawal.
§ Rationale: May
indicate onset of depression (common after effect of stroke), which may require
further evaluation and intervention.
§ Refer
for neuropsychological evaluation and/or counseling if indicated.
§ Rationale: May
facilitate adaptation to role changes that are necessary for a sense of
feeling/being a productive person. Note: Depression is common in stroke
survivors and may be a direct result of the brain damage and/or an emotional
reaction to sudden-onset disability.
Nursing Diagnosis
§ Self-Care
Deficit
May be related to
§ Neuromuscular
impairment, decreased strength and endurance, loss of muscle
control/coordination
§ Perceptual/cognitive
impairment
§ Pain/discomfort
§ Depression
Possibly evidenced by
§ Impaired
ability to perform ADLs, e.g., inability to bring food from receptacle to
mouth; inability to wash body part(s), regulate temperature of water; impaired
ability to put on/take off clothing; difficulty completing toileting tasks
Desired Outcomes
§ Demonstrate
techniques/lifestyle changes to meet self-care needs.
§ Perform
self-care activities within level of own ability.
§ Identify
personal/community resources that can provide assistance as needed.
Nursing Interventions
§ Assess
abilities and level of deficit (0–4 scale) for performing ADLs.
§ Rationale: Aids
in planning for meeting individual needs.
§ Avoid
doing things for patient that patient can do for self, but provide assistance
as necessary.
§ Rationale: To
maintain self-esteem and promote recovery, it is important for the patient to
do as much as possible for self. These patients may become fearful and
independent, although assistance is helpful in preventing frustration.
§ Be
aware of impulsive actions suggestive of impaired judgment.
§ Rationale: May
indicate need for additional interventions and supervision to promote patient
safety.
§ Maintain
a supportive, firm attitude. Allow patient sufficient time to accomplish tasks.
Don’t rush the patient.
§ Rationale: Patients
need empathy and to know caregivers will be consistent in their assistance.
§ Provide
positive feedback for efforts and accomplishments.
§ Rationale: Enhances
sense of self-worth, promotes independence, and encourages patient to continue
endeavors.
§ Create
plan for visual deficits that are present: Place food and utensils on the tray
related to patient’s unaffected side; Situate the bed so that patient’s
unaffected side is facing the room with the affected side to the wall; Position
furniture against wall/out of travel path.
§ Rationale: Patient
will be able to see to eat the food. Will be able to see when getting in/out of
bed and observe anyone who comes into the room. Provides for safety when
patient is able to move around the room, reducing risk of tripping/falling over
furniture.
§ Provide
self-help devices: extensions with hooks for picking things up from the floor,
toilet risers, long-handled brushes, drinking straw, leg bag for catheter,
shower chair. Encourage good grooming and makeup habits.
§ Rationale: To
enable the patient to manage for self, enhancing independence and self-esteem,
reduce reliance on others for meeting own needs, and enables the patient to be
more socially active.
§ Encourage
SO to allow patient to do as much as possible for self.
§ Rationale: Reestablishes
sense of independence and fosters self-worth and enhances rehabilitation
process. Note: This may be very difficult and frustrating for the
caregiver, depending on degree of disability and time required for patient to
complete activity.
§ Assess
patient’s ability to communicate the need to void and/or ability to use urinal,
bedpan. Take patient to the bathroom at periodic intervals for voiding if
appropriate.
§ Rationale: Patient
may have neurogenic bladder, be inattentive, or be unable to communicate needs
in acute recovery phase, but usually is able to regain independent control of
this function as recovery progresses.
§ Identify
previous bowel habits and reestablish normal regimen. Increase bulk in diet,
encourage fluid intake, increased activity.
§ Rationale: Assists
in development of retraining program (independence) and aids in preventing
constipation and impaction (long-term effects).
§ Teach
the patient to comb hair, dress, and wash.
§ Rationale: To
promote sense o f independence and self-esteem.
§ Refer
patient to physical and occupational therapist.
§ Rationale: Rehabilitation
helps to relearn skills that are lost when part of the brain is damaged. It
also teaches new ways of performing tasks to circumvent or compensate for any
residual disabilities.





{kind=link}
{kind=link}
0 comments:
Post a Comment